Carolyn Devine
Carolyn Devine
Certified Woofer!

(Woofer is how outdoor professionals refer to a Wilderness First Responder, or WFR)
It’s been 10 days of approximately 30 scenarios (including one multi-hour rescue at night); lectures on trauma, human physiology and what goes wrong in the wilderness; lots of practice making splints, CPR, checking blood pressures; and not much time for regular daily living: laundry, cooking, blogging, and getting exercise other than putting on layers to go outside and play patient or rescuer.
Fun, exhausting, stressful, challenging, information-packed.
The outcome?
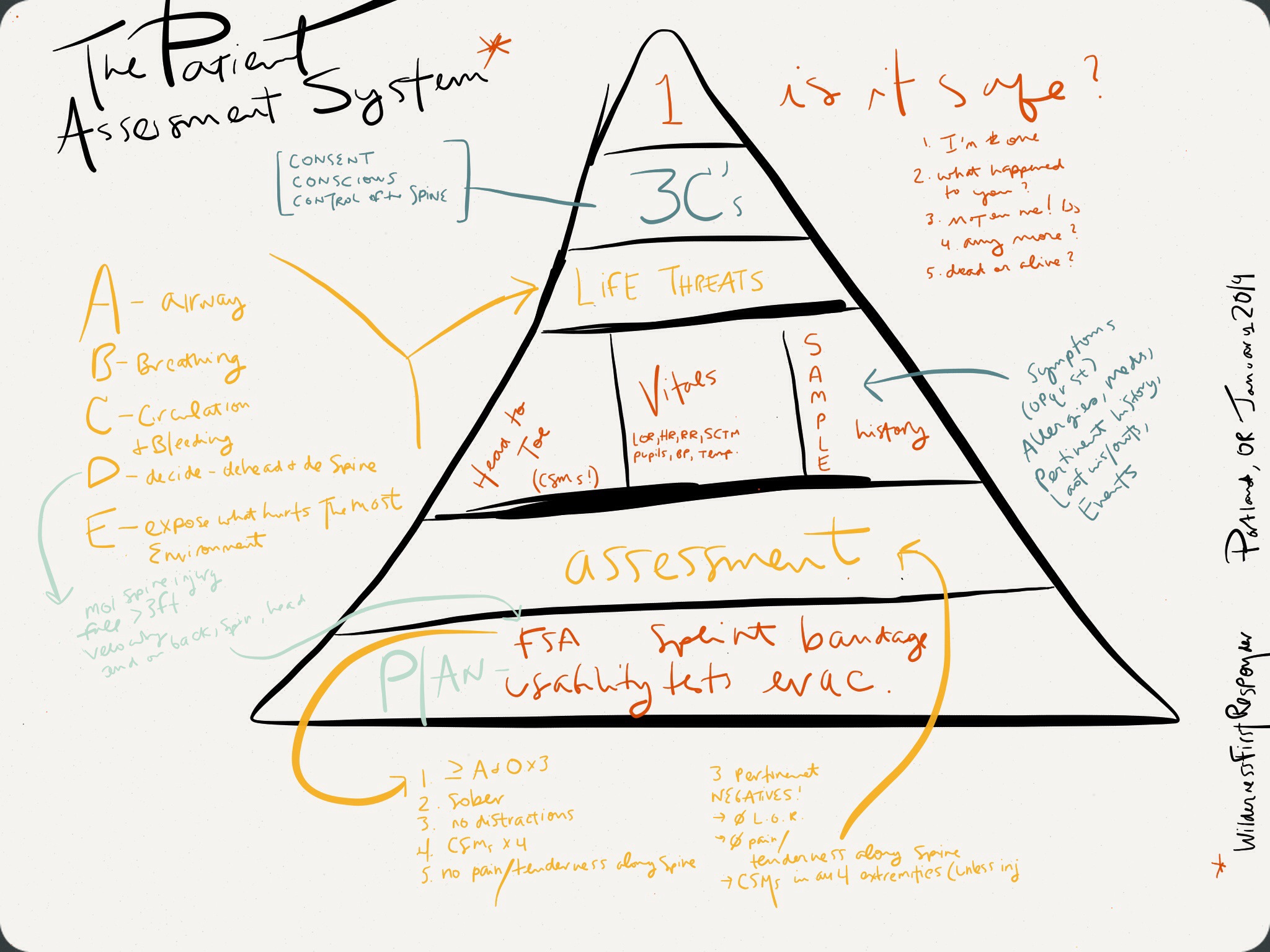
I feel confident that if I’m more than 1 hour away from professional emergency care and I should come across a hiker on the trail, I’d be able to methodically go through the “Patient Assessment System” to:
- • Size up the scene (safe to help? what happened? how many hurt?)
- • Determine whether or not the hiker is facing a life threat
- • Determine whether or not the hiker is facing a spinal injury threat
- • Collect important pertinent data for informed decision-making about the need for evacuation (and how rapid)
- • Improvise short-term solutions to manage trauma (wounds, first signs of shock, fractures, dislocations, etc.) until a rescue comes
- • Safely transport someone should that be necessary
- • Communicate my findings to definitive care succinctly and in an outline that would make sense to them.
Valuable stuff that I hope I won’t have to use.
Why I am glad I chose Wilderness First Responder vs. Wilderness First Aid?
Before choosing this investment in time and money, I did some research and decided that WFA wouldn’t provide me with much more information than my urban First Aid Certification.
For Wilderness First-Aiders, Check/Call/Care simply becomes Check/Care (only a bit)/Wait for help.
WFRs practice the patient assessment system daily. We learned a few pieces of care that we would never do in an urban setting but could help in the wilderness. To my estimation, the most important of these is the: Focused Spinal Assessment.
Scenario: You suspect a possible spine injury (the fall was more than 3 feet, and/or at a high velocity, and/or the patient landed on the head, spine, or butt).
WFA: You’re stuck. Your obligation (unless the scene becomes unsafe) is to stabilize the spine and hold the head in place until definitive care arrives. That could be a while.
WFR: You complete the Patient Assessment System, and then perform a Focused Spine Assessment. If all goes well, you can release spine stabilization. Which makes things a lot lot better. They can be treated easier and even walk out. Furthermore, I can see myself (and my previously frost-bitten toes / Raynaud’s syndrome-prone extremities) being stuck with the decision of having to leave someone in order to keep myself warm and safe.
Other WFR specific (rather than WFA) skills include:
- • reducing dislocations of these 5 kind: anterior shoulder, jaw, fingers, toes, patella
- • traction in line for a mid-femur fracture – this is controversial, apparently, but it seems like if you do it correctly, it’s better than not doing it (I’d like some research on this).
- • the Focused Spine Assessment (FSA for short) – a powerful tool and could come in handy.
Overall, a great class. Bethany and Erik were some of the best instructors I’ve ever had. They demonstrated perfect pacing, a good mix of compassion and humor, front-loaded topics to prevent conversations getting off track, and demonstrated polite but firm classroom management to keep us focused. They were top notch!